Guidelines Updates for Opportunistic Infections in Adults with HIV
Opportunistic HIV infections (OIs) are infectious diseases that exploit the weakened immune system in people with HIV (Human Immunodeficiency Virus). Prior to effective antiretroviral therapy (ART), OIs were usually the first signs of AIDS, often leading to a life expectancy of only 1 to 2 years post-diagnosis. In the late 1980s, advancements in managing OIs emerged, followed by improved treatments and early antiretroviral medications that increased survival rates.1 However, the most significant reduction in OIs occurred with highly effective combination ART in the mid-1990s. Despite progress and the availability of efficient ART regimens, many challenges regarding OIs persist. Therefore, it remains crucial for healthcare providers to stay informed about the prevention and management of HIV-related OIs.
One effective way for healthcare providers to stay informed about the prevention and management of HIV-related OIs is by following established guidelines. These guidelines serve as essential references, offering up-to-date recommendations and strategies for the care of individuals living with HIV. They provide a wealth of information on the prevention, diagnosis, and treatment of OIs, helping healthcare providers deliver the best possible care. The most recent updates to the Guidelines for the Prevention and Treatment of Opportunistic Infections in Adults and Adolescents with HIV have brought about significant changes in key areas. Notably, updates regarding syphilis and immunizations have been made in September 2023. These changes aim to enhance prevention and management strategies for individuals with HIV, reflecting the evolving landscape of care and the importance of up-to-date recommendations.
Syphilis is a sexually transmitted infection (STI) caused by the bacterium Treponema pallidum. It is a complex and potentially severe disease that progresses through several stages if left untreated. Syphilis is known for its variable and sometimes subtle symptoms, which makes diagnosis and management challenging. This STI can affect various organ systems, including the skin, mucous membranes, internal organs, and the central nervous system. In addition to its clinical impact, the presence of syphilis in individuals with HIV is associated with an increased risk of sexual acquisition and transmission of HIV. Managing syphilis in this context requires careful consideration and adherence to specific treatment regimens.
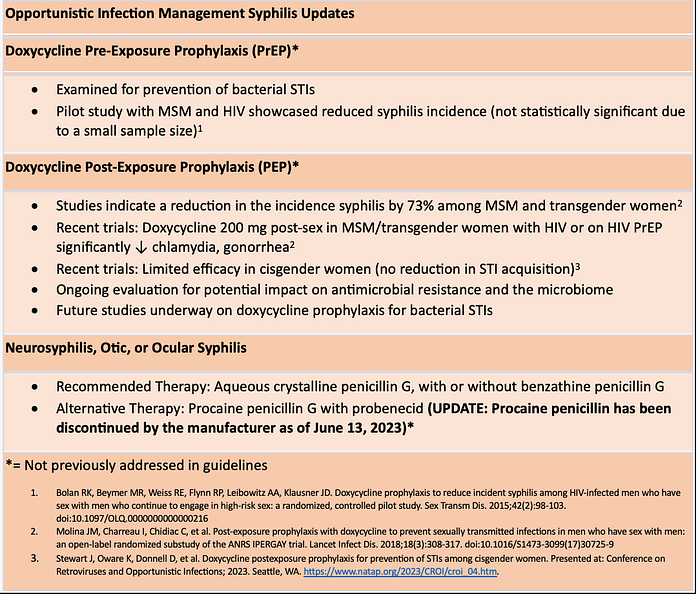
The guidelines for the Prevention and Treatment of Opportunistic Infections in Adults and Adolescents with HIV include changes in recommendations regarding the management of syphilis. The updated guidelines have accounted for emerging research on the use of doxycycline for pre-exposure and post-exposure prophylaxis against bacterial sexually transmitted infections. A pilot study involving 30 men who have sex with men (MSM) with HIV and prior syphilis infections revealed a randomized assignment to a 100 mg daily doxycycline regimen for 48 weeks. This study compared doxycycline to a financial incentive-based behavioral intervention and found that doxycycline was associated with a lower incidence of syphilis. However, it’s essential to note that the reduced incidence did not reach statistical significance due to the small sample size.
In the context of post-exposure prophylaxis, the guidelines also consider doxycycline’s role. Studies involving MSM and transgender women have indicated a 73% reduction in incident syphilis when doxycycline is administered at a dose of 200 mg after unprotected anal sex. Recent randomized open-label clinical trials further support the effectiveness of doxycycline, specifically at a 200 mg dose, after condomless sex among MSM and transgender women with HIV or on HIV PrEP.3 This approach has demonstrated significant reductions in the acquisition of chlamydia, gonorrhea, and syphilis. Interestingly, a randomized trial involving cisgender women on HIV PrEP who received doxycycline at a 200 mg dose within 72 hours after sex did not show a reduction in the acquisition of these STIs.
The guidelines also address the ongoing evaluation of the potential impact of STI postexposure prophylaxis on antimicrobial resistance and the microbiome. This area is actively being investigated to ensure that the use of doxycycline as prophylaxis is as effective and safe as possible. Additionally, the guidelines acknowledge that various studies are currently underway or in development regarding the use of doxycycline for prophylaxis against bacterial STIs. This reflects the evolving landscape of STI prevention and underscores the importance of staying informed about the latest research findings and recommendations.[MS1]
When it comes to the general considerations for treating syphilis, specific considerations are made regarding the choice of penicillin preparations. The guidelines emphasize the importance of selecting the appropriate penicillin formulation due to the potential sequestration of Treponema pallidum in less accessible sites, such as the central nervous system (CNS) and aqueous humor. Notably, combinations of oral benzathine penicillin and procaine penicillin or short-acting benzathine-procaine penicillin (Bicillin C‑R) preparations are discouraged for syphilis treatment. The recommendations stress that the efficacy of non-penicillin alternatives, especially in individuals with HIV, requires close clinical and serologic monitoring. Furthermore, the guidelines address a notable phenomenon known as the Jarisch-Herxheimer reaction, an acute febrile reaction accompanied by symptoms like headache, fever, and myalgias. This reaction can occur within the first 24 hours after syphilis therapy, more commonly in individuals with early-stage syphilis. Importantly, it can have consequences such as early labor or fetal distress during pregnancy. Therefore, it is essential for healthcare providers to educate patients about this potential reaction to penicillin treatment and clarify that it is not an allergic response to penicillin.
The management of syphilis varies according to the disease’s stage. In early-stage syphilis (primary, secondary, and early latent syphilis within the first year), the recommended therapy remains a single dose of 2.4 million units of intramuscular benzathine penicillin G. For individuals with penicillin allergies, alternative treatments, such as doxycycline or ceftriaxone, are suggested. However, it’s essential that those with penicillin allergies who have syphilis during pregnancy undergo penicillin desensitization and treatment with benzathine penicillin. The guidelines also highlight a potential second dose of benzathine penicillin G for pregnant individuals to prevent congenital syphilis effectively.
Late latent syphilis (lasting longer than 1 year) or latent syphilis of unknown duration warrants a three-dose regimen of benzathine penicillin G administered weekly. For individuals with penicillin allergies, doxycycline is recommended, with an emphasis on the importance of patient compliance and follow-up to ensure successful treatment. In cases of late-stage syphilis, particularly tertiary syphilis presenting as cardiovascular or gummatous disease, a cerebrospinal fluid examination is essential to guide management. Treatment strategies differ based on the presence of neurosyphilis, with those without neurosyphilis recommended to receive a weekly regimen of benzathine penicillin G. On the other hand, neurosyphilis, otic, or ocular syphilis necessitates treatment with aqueous crystalline penicillin G, potentially followed by a single injection of benzathine penicillin G. However, it’s crucial to note that procaine penicillin G, which was formerly an alternative, has been discontinued by the manufacturer, prompting the need for other treatment options.
For penicillin-allergic individuals with neurosyphilis, otic or ocular syphilis, desensitization to penicillin is the preferred approach. In cases where desensitization is not feasible, and the patient is not pregnant, alternative therapy using ceftriaxone is recommended. It’s also worth considering that individuals with a history of IgE-mediated penicillin hypersensitivity may lose their sensitivity after 10 years, potentially allowing for a negative skin test evaluation followed by an oral challenge. These comprehensive recommendations aim to ensure effective prevention and treatment of syphilis in individuals with HIV while considering various scenarios and risk factors.
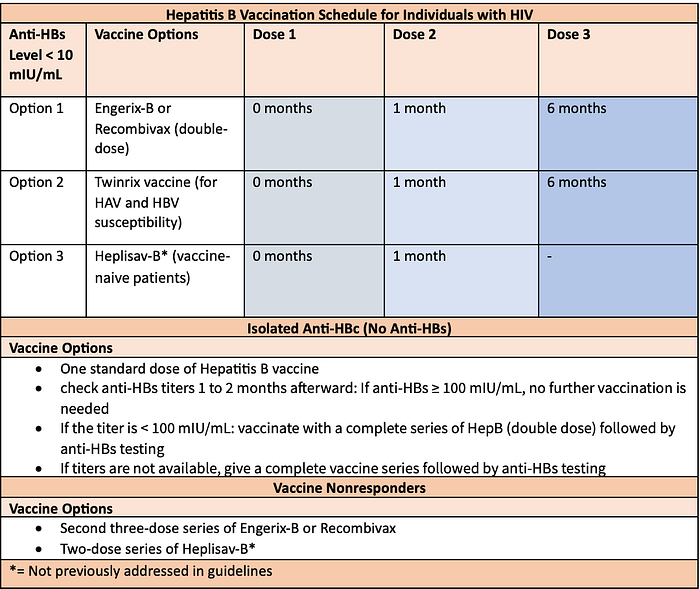
In addition to these recent updates on Syphilis management, The Guidelines for the Prevention and Treatment of Opportunistic Infections in Adults and Adolescents with HIV provide revised recommendations for three key vaccines: Hepatitis B Vaccine, Meningococcal Vaccine, and Pneumococcal Vaccine. The updated guidelines provide a comprehensive approach to Hepatitis B vaccination for individuals with HIV who are susceptible to HBV. If their anti-HBs (Hepatitis B surface antibody) level is less than 10 mIU/mL, they have several vaccination options. These individuals can choose to receive a “double-dose” three-dose series of Engerix-B (40 mcg; two injections of 20 mcg each) or Recombivax ( 20 mcg; two injections of 10 mcg each) at 0, 1, and 6 months. An alternative for those susceptible to both HAV and HBV is the Twinrix vaccine, a three-dose series given at 0, 1, and 6 months. There’s also the Heplisav option, a two-dose series administered at 0 and 1 month. It is important to obtain anti-HBs levels 1 to 2 months after completing the vaccine series. In cases of isolated anti-HBc (Hepatitis B core antibody) with no anti-HBs, individuals should receive a standard dose of Hepatitis B vaccine, followed by anti-HBs testing. Safety and efficacy of Heplisav have not been studied in people with HIV, but it remains an option for those who prefer a two-dose vaccine series. In cases of significant delays between vaccine doses, there’s no need to restart the series. Additionally, the guidelines do not recommend double-dose Engerix-B or Recombivax for individuals with HIV. For vaccine nonresponders, revaccination options include a second three-dose series of Engerix-B or Recombivax or a two-dose series of Heplisav-B, with the caution to delay repeat vaccination until CD4 counts are at least 200 cells/mm³. Post-exposure prophylaxis recommendations vary based on vaccination history and potential exposure.
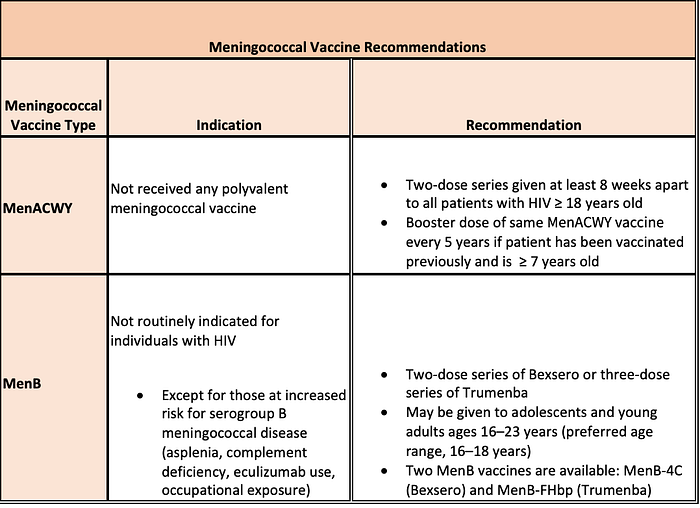
The guidelines also emphasize the importance of meningococcal vaccination for individuals with HIV. Meningococcal meningitis, caused by Neisseria meningitidis, poses a considerable risk for this population. To address this risk, the guidelines recommend that two doses of the quadrivalent meningococcal conjugate vaccine should be administered to all individuals with HIV who are 18 years of age or older, and these doses should be spaced at least 8 weeks apart. For individuals with HIV who are undergoing primary vaccination, the guidelines further emphasize the importance of administering two doses of the quadrivalent meningococcal conjugate vaccine, also separated by at least 8 weeks to ensure an optimal immune response. Additionally, for individuals with HIV who have previously received meningococcal vaccination and are aged 7 years or older, a repeat vaccination every 5 years throughout their life is advised. It is noteworthy that, as of the current guidelines, routine serogroup B meningococcal vaccination (MenB) is not recommended for adults and adolescents with HIV.
There is a growing body of evidence indicating an elevated risk of meningococcal disease among individuals with HIV. Several studies have highlighted this risk, demonstrating a 5- to 24-fold increase in the prevalence of meningococcal disease in those with HIV compared to those without the virus.[MS1] 5 Moreover, it has been observed that individuals with a lower CD4 count and higher HIV viral load are at a greater risk of invasive meningococcal disease. The annual incidence rate of invasive meningococcal disease was reported at 0.39 cases per 100,000 people.6 Notably, individuals with lower CD4 counts are at a higher risk of invasive disease. Studies also shed light on the low uptake of MenACWY vaccination among individuals newly diagnosed with HIV. Additionally, the time to receiving the first vaccination in this group was often prolonged, emphasizing the need to enhance vaccination rates and timing.[MS2] 7
Regarding vaccine safety and efficacy, MenACWY-D has been evaluated in individuals with HIV aged 11 to 24 years. Those with CD4 percentages equal to or greater than 15% received either one or two doses, while those with CD4 percentages less than 15% received two doses. Encouragingly, 21% to 63% of individuals who received a single dose developed an antibody titer of 1:128 or higher at 72 weeks post-vaccination. However, in those with CD4 percentages below 15%, only 6% to 28% achieved similar titers. The vaccine exhibited a low frequency of local site reactions (3.1%) and grade 3 or greater adverse events (2.2%), with no vaccine-related deaths or instances of meningitis reported. Importantly, there is a lack of safety and immunogenicity studies for MenACWY-CRM in individuals with HIV, and clinical outcome data for both vaccines in this population remain limited.
There have been reported outbreaks of meningococcal meningitis among men who have sex with men in the United States, involving individuals both with and without HIV. These outbreaks have led some public health jurisdictions to recommend meningococcal vaccination for all men who have sex with men, regardless of their HIV status. However, it’s crucial to note that the Advisory Committee on Immunization Practices has not adopted this recommendation for men who have sex with men without HIV currently. These findings and recommendations highlight the critical importance of meningococcal vaccination for individuals with HIV and the necessity to address vaccination gaps and risk factors.
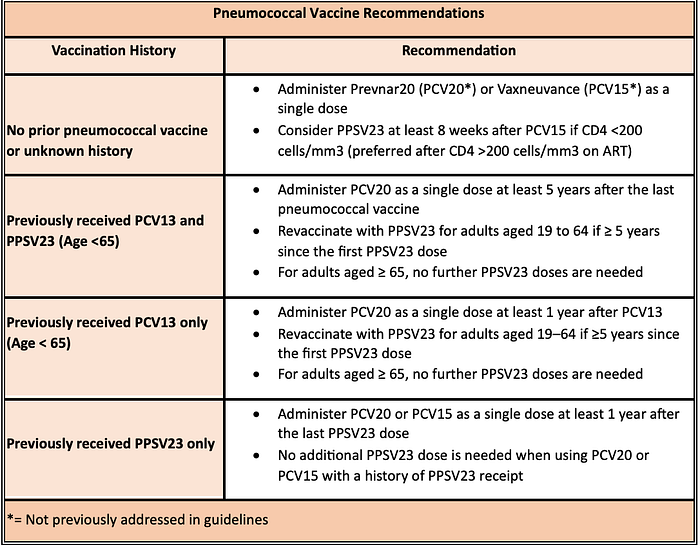
Lastly, the guideline updates also provide recommendations for pneumococcal vaccination in people with HIV, focusing on different scenarios. For individuals with HIV who have not been previously vaccinated against pneumococcal infections or have an unknown vaccination history, the guidelines recommend administering either the 20-valent pneumococcal conjugate vaccine (PCV20) or the 15-valent pneumococcal conjugate vaccine (PCV15). In cases where PCV15 is used, a dose of the 23-valent pneumococcal polysaccharide vaccine (PPSV23) should be administered at least eight weeks later, with no further pneumococcal vaccine doses recommended. The guidelines emphasize that those who have already initiated or completed a pneumococcal vaccination series should not restart the series. The recommendations differ based on the age and specific vaccines received. For individuals with HIV who received the 13-valent pneumococcal conjugate vaccine (PCV13) and were 65 years or older at the time of receiving a dose of PPSV23, additional PPSV23 doses are not necessary. However, clinical judgment is advised for those aged 65 or older who completed their vaccine series with both PCV13 and PPSV23, with a suggested PCV20 dose at least five years after the last pneumococcal vaccine dose. If individuals with HIV received PCV13 and were younger than 65 when they received a dose of PPSV23, the guidelines suggest one dose of PCV20 administered at least five years after their previous pneumococcal vaccinations. Alternatively, additional doses of PPSV23 may be recommended in specific situations.
In cases where individuals with HIV have only received PPSV23, they may receive a pneumococcal conjugate vaccine (either PCV20 or PCV15) at least one year after their last PPSV23 dose, allowing them to complete their pneumococcal vaccination series. For individuals who had previously received only PCV13, the guidelines suggest either receiving one dose of PCV20 at least one year later or receiving PPSV23 at least eight weeks later, followed by the completion of the PPSV23 series as recommended earlier. These recommendations aim to provide comprehensive pneumococcal protection for individuals living with HIV, considering their specific vaccination history and age, to reduce the risk of pneumococcal infections.
These guideline recommendations for the prevention and treatment of OIs in adults and adolescents with HIV play a vital role in safeguarding the health of this vulnerable population. OIs are a persistent concern for those with HIV, but the continuous evolution of guidelines offers hope and proactive strategies for addressing these challenges. Healthcare providers play a crucial role in implementing these recommendations and it is important to stay updated to provide the highest standard of care and improve the well-being of individuals with HIV.
Written by Drug Information Fellow: Muna Said, PharmD
References:
1. HIV Clinical Guidelines: Adult and Adolescent Opportunistic Infections — What’s New in the Guidelines. Clinicalinfo.HIV.gov. clinicalinfo.hiv.gov. Published September 25, 2023. Accessed October 20, 2023. https://clinicalinfo.hiv.gov/en/guidelines/hiv-clinical-guidelines-adult-and-adolescent-opportunistic-infections/whats-new?view=full
2. Bolan RK, Beymer MR, Weiss RE, Flynn RP, Leibowitz AA, Klausner JD. Doxycycline prophylaxis to reduce incident syphilis among HIV-infected men who have sex with men who continue to engage in high-risk sex: a randomized, controlled pilot study. Sex Transm Dis. 2015;42(2):98–103. doi:10.1097/OLQ.0000000000000216
3. Molina JM, Charreau I, Chidiac C, et al. Post-exposure prophylaxis with doxycycline to prevent sexually transmitted infections in men who have sex with men: an open-label randomised substudy of the ANRS IPERGAY trial. Lancet Infect Dis. 2018;18(3):308–317. doi:10.1016/S1473–3099(17)30725–9
4. Stewart J, Oware K, Donnell D, et al. Doxycycline postexposure prophylaxis for prevention of STIs among cisgender women. Presented at: Conference on Retroviruses and Opportunistic Infections; 2023. Seattle, WA. https://www.natap.org/2023/CROI/croi_04.htm.
5. Harris CM, Wu HM, Li J, et al. Meningococcal Disease in Patients With Human Immunodeficiency Virus Infection: A Review of Cases Reported Through Active Surveillance in the United States, 2000–2008. Open Forum Infect Dis. 2016;3(4):ofw226. Published 2016 Dec 20. doi:10.1093/ofid/ofw226
6. Miller L, Arakaki L, Ramautar A, et al. Elevated risk for invasive meningococcal disease among persons with HIV. Ann Intern Med. 2014;160(1):30–37. doi:10.7326/0003–4819–160–1–201401070–00731
7. Ghaswalla PK, Marshall GS, Bengtson LGS, et al. Meningococcal Vaccination Rates Among People With a New Diagnosis of HIV Infection in the US. JAMA Netw Open. 2022;5(4):e228573. Published 2022 Apr 1. doi:10.1001/jamanetworkopen.2022.8573
